Wellington stop-smoking provider Takiri Mai Te Ata Trust ended its partnership with Health New Zealand after refusing to promote vaping as a smoking cessation tool. The trust, which has helped people quit smoking for more than 30 years, said it could not continue delivering services in a way that conflicted with its values. Regional manager Catherine Manning said the organization did not support helping people quit cigarettes by transitioning to another nicotine product.
Health New Zealand said it worked extensively with the trust to find a solution that would allow the service to continue without directly supplying vapes, but no agreement was reached, and the contract ended by mutual consent. Health New Zealand maintains that vaping is less harmful than smoking and can help smokers quit, while stressing that non-smokers should not vape. Action for Smokefree 2025 director Ben Youdan said evidence shows vaping can be an effective cessation tool, adding that vaping is “not risk-free” but “dramatically” reduces the risk of death compared with smoking.
Youdan said that while he recognized the trust’s concerns, many organizations have seen real benefits from using vaping as part of smoking cessation efforts.
The Coalition of Asia Pacific Tobacco Harm Reduction Advocates is urging governments across the Asia-Pacific region to review the U.S. Food and Drug Administration’s recent authorization allowing 20 Zyn nicotine pouch products to carry reduced-risk claims for adult smokers. CAPHRA said the FDA’s decision recognizes the principle of relative risk following scientific review and should encourage regulators to distinguish between combustible cigarettes, high-risk smokeless tobacco products, and lower-risk smoke-free nicotine alternatives.
The group called on policymakers to adopt evidence-based, risk-proportionate regulation, strengthen youth access restrictions and product standards, and ensure adult consumers receive accurate information about the comparative risks of nicotine products, arguing that treating all nicotine products as equally harmful undermines public health objectives.
A survey of 1,973 U.S. adults commissioned by Haypp Group, parent of Nicokick.com and Northerner, found most respondents do not distinguish between the health risks of cigarettes and non-combustible nicotine products. According to the Nicotine Product Harm Perception Report 2026, 73% said vaping is as harmful as, or more harmful than, smoking; 60.6% said the same of nicotine pouches, and 64.9% incorrectly believed nicotine causes cancer.
While 68.9% of respondents said they feel informed about nicotine risks, many answers conflicted with established evidence that combustion, not nicotine, is the primary cause of smoking-related disease. The survey also found that younger adults perceive smoking as more culturally visible, with 36.3% of those aged 25–34 saying smoking is “back in fashion,” even as U.S. smoking rates have fallen to about 9.9% in 2024.
Three former directors at the World Health Organization say a global smoking rate below 5% by 2040 is achievable if tobacco harm reduction is formally integrated into the WHO Framework Convention on Tobacco Control. Writing in Nature Health recently, Robert Beaglehole, Ruth Bonita, and Tikki Pang argued that progress in reducing smoking has slowed in many high-burden countries and that current policy debates increasingly conflate nicotine use with the harms of smoking. They called for a “risk-proportionate regulatory framework” that maintains strict controls on combustible tobacco while allowing regulated access to smoke-free alternatives that can displace cigarettes without encouraging youth uptake.
The authors pointed to examples including Japan, Sweden, and New Zealand, where wider adoption of heated tobacco, snus, nicotine pouches, and vaping coincided with sharp declines in smoking rates. Former WHO director Derek Yach described the commentary as significant but questioned whether large, high-smoking countries would follow those models. The paper maintains that combining established FCTC measures with broader access to regulated smoke-free products offers the most realistic path toward the 2040 goal, even as current FCTC leadership has shown little openness to revisiting its stance on harm reduction.
Why the World Cannot Afford America’s Regulatory Model
By Dr. J. Preston Campbell, Cancer Researcher, Harm Reduction Scientist
Heavy lifetime smoking kills approximately half of long-term users. That is not a projection or a model output — it is one of the most replicated findings in twentieth-century epidemiology, confirmed across decades and continents (WHO, 2023). In the United States alone, tobacco-attributable disease generates an estimated $310 billion in annual healthcare costs, roughly $6,500 per smoker per year (Xu et al., 2015; ASH, 2021). Globally, the burden exceeds $1.4 trillion annually (WHO, 2023). We know what is causing the damage. We have products that demonstrably reduce it. The question worth asking — the one this analysis is organized around — is why those products cost 167 times more per life saved to bring to market in the United States than in the European Union.
The Health Economics Punchline
Nicotine pouches are, by most objective measures, one of the less scientifically interesting harm- reduction products ever developed. No combustion. No inhalation. No tobacco leaf. Pharmaceutical-grade nicotine salt in a cellulose pouch placed between lip and gum for thirty minutes. Peer-reviewed toxicant studies document 95–99% lower exposure to carcinogens compared to cigarettes (Mallock et al., 2019; Snusforumet, 2021). The first Cochrane systematic review, published October 2025, found no serious adverse events across all trials and confirmed consistently reduced toxicant biomarkers in every switching cohort studied (Hartmann-Boyce et al., 2025). The product’s risk profile is not controversial. What is controversial, apparently, is the cost of allowing it to be sold.
The standard health-economic metric for evaluating interventions is cost per quality-adjusted life year (QALY) gained — a single number that combines how long and how well someone lives. The U.S. cost-effectiveness threshold is $50,000–$100,000 per QALY. Published ICER estimates for comparable nicotine delivery products run $7,500/QALY for NRT sampling programs and $11,454/QALY for e-cigarettes used as cessation aids (Maciosek et al., 2022; Masiero et al., 2025). Based on the observed 5.2% switch rate in national survey data and the documented 95% risk reduction from switching, nicotine pouches are estimated to fall in the $3,000–$15,000/QALY range — well inside the cost-effectiveness frontier by any standard (Delnevo et al., 2024; Goniewicz et al., 2025).
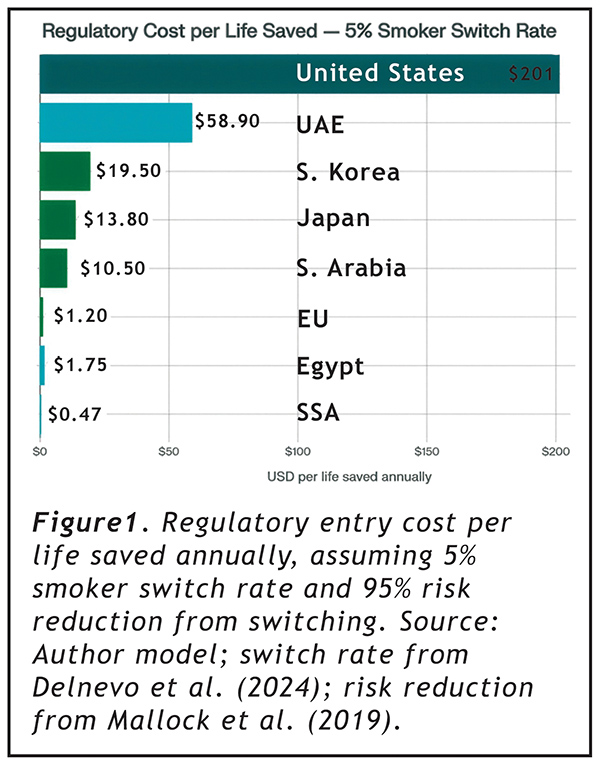
At that switch rate, applying regulatory entry costs to the lives saved annually from harm reduction produces Figure 1.
The U.S. costs $201 per statistical life saved per year. The EU costs $1.20. Sub-Saharan Africa costs $0.47. These numbers do not argue that FDA should wave products through without review. They argue something more specific: that a regulatory framework costing 167 times more per life saved than its closest comparator is not optimizing for public health outcomes. It is optimizing for something else.
Why: The Entry Cost Structure
The reason is straightforward once the numbers are placed side by side.
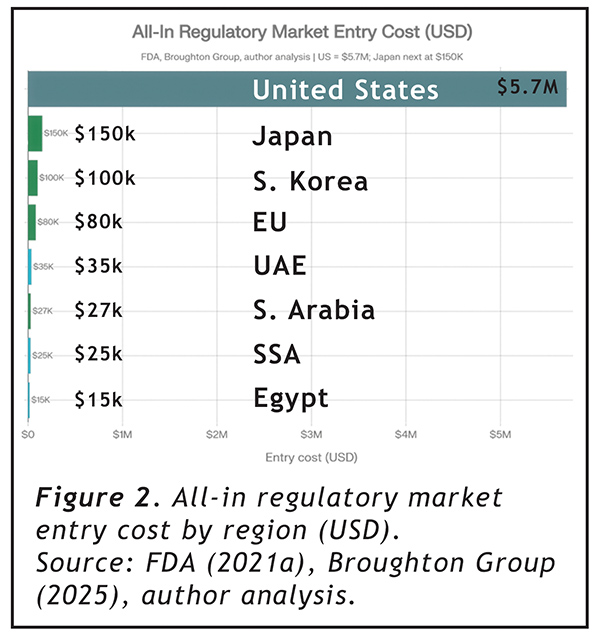
In the United States, bringing a single nicotine pouch product line to market requires a Premarket Tobacco Application. FDA’s own published cost estimate of $117,000–$466,563 per application (FDA, 2021a) has not aged well. Industry experience places the all-in cost at $4.2–$7.2 million per product family, once pharmacokinetic trials ($1M+), 12-month stability studies ($250K+), consumer perception research, addiction liability assessments, and regulatory consulting are properly accounted for (Broughton Group, 2025; JJCC Group, 2026). ZYN’s January 2025 marketing authorization — the first for this product class — took years and the resources of a Fortune 500 company (FDA, 2025a).
Elsewhere, the numbers describe a different regulatory universe. EU notification under the Tobacco Products Directive: $30,000–$80,000 per market. UAE ECAS registration: $35,000. Saudi Arabia: $27,000. Egypt — an open market of 14.5 million smokers — $15,000 (Broughton Group, 2025; SGS, 2025; author analysis). A company could simultaneously enter the EU’s 110 million-smoker market, Japan, South Korea, UAE, Saudi Arabia, Egypt, and sub-Saharan Africa for less than one U.S. PMTA submission.
Why It Is Worse Than It Looks:The Time Factor
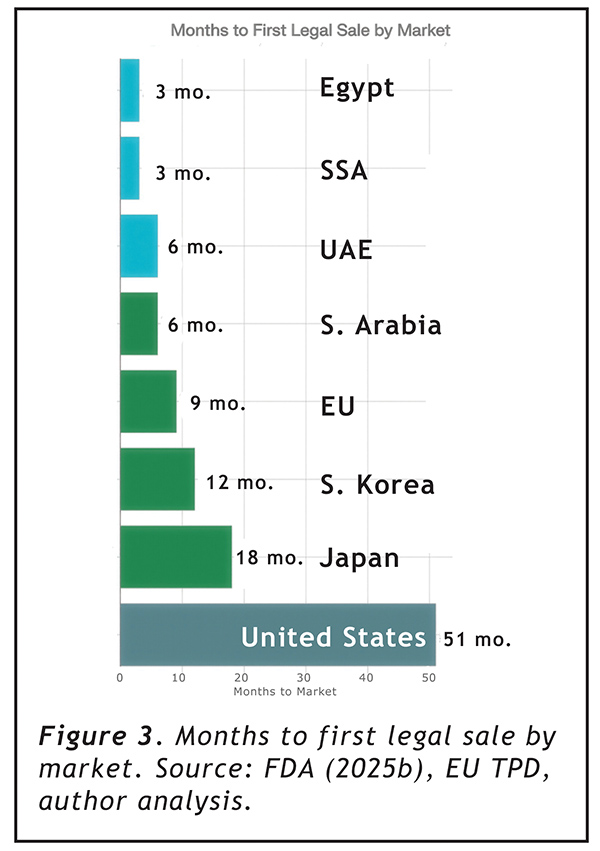
Entry cost alone understates the problem. The PMTA requires a minimum of 15 months of mandatory studies before submission, followed by an FDA review period averaging over three years to date (FDA, 2025b; Tobacco Law Blog, 2025). From the date a company decides to enter the U.S. market, the minimum realistic timeline to first legal sale is 51 months — over four years. The EU takes 9 months. The UAE and Saudi Arabia: 6 months. Egypt and sub-Saharan Africa: 3 months (author analysis).
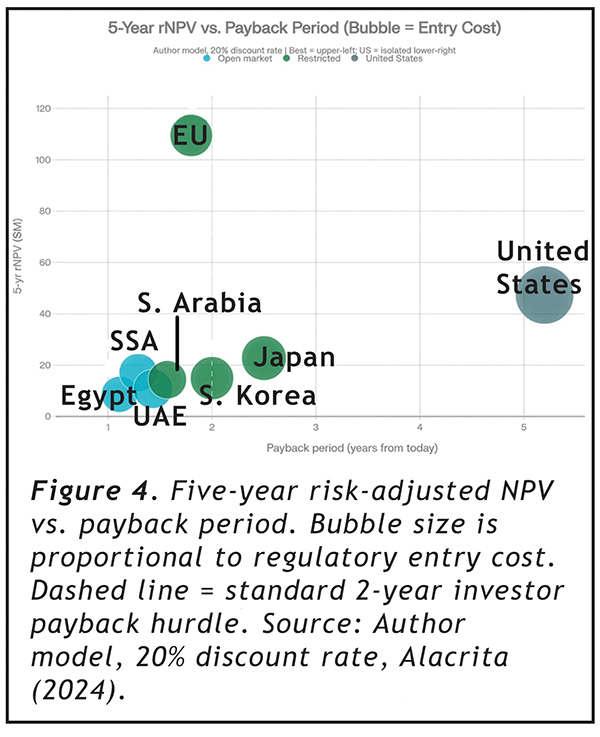
When those timelines are applied to financial models — discounting future revenue at the 20% rate typical for early-stage consumer products and adjusting for denial risk (estimated at 35% for new U.S. entrants; FDLI, 2023) — the picture becomes harder to rationalize from any direction.
The EU, despite having roughly half the U.S. annual revenue potential, generates a 5-year risk-adjusted NPV of $109.5 million compared to the U.S. at $47.3 million — because it begins generating cash 42 months earlier at one-tenth the cost. The U.S. payback period from today to regulatory cost recovery is 5.2 years, compared to 1.8 years for the EU and 1.2 years for Egypt. The U.S. is the only market in this analysis that exceeds the standard 2-year payback threshold that most venture and growth-equity investors apply to consumer product categories (Alacrita, 2024). During the 48-month excess waiting period, a company forfeits approximately $270 million in gross margin that would otherwise accrue in markets where the same product is already legally sold.
The 5-year ROI multiple on regulatory spend, risk-adjusted: 55× for the U.S., compared to 3,135× for the EU and 1,465× for sub-Saharan Africa. The PMTA does not just cost more — it structurally consumes the financial return from market participation, leaving only companies with institutional balance sheets able to absorb it.
The Cessation Paradox FDA Built
Here is where it gets genuinely strange.
FDA’s own authorization of ZYN stated explicitly that the products “have the potential to provide a benefit to adults who smoke cigarettes and would like to switch to a lower-risk alternative” (FDA, 2025a). The PMTA submissions included cessation and switching behavior data. FDA reviewed them. FDA relied on them to issue authorization.
And then FDA’s post-authorization communications carefully noted that the products are “not FDA approved” and that “there is no safe tobacco product” — language that systematically prevents companies from communicating the public health rationale that justified the authorization (FDA, 2025a).
Under the Tobacco Control Act, tobacco products cannot make cessation claims. If a company wants to say anything about reduced risk, it must file a separate Modified Risk Tobacco Product application — another process, more years, more millions, with public comment periods, advisory committee referrals, and post-market surveillance requirements (FDA, 2025c). As of 2024, FDA had received 48 MRTP applications since 2010 and authorized exactly 16 products (LDI Penn, 2025).
The logic chain deserves a slow read: FDA required switching studies as a PMTA condition. It reviewed them. It relied on them to grant authorization. It then prohibited companies from telling consumers those studies existed. The MRTP pathway functions in practice as a second admission ticket for a claim FDA already accepted as scientifically valid during the PMTA review. This is not a minor regulatory inconvenience. It is the architecture of a system in which harm reduction is simultaneously required as scientific evidence and forbidden as commercial communication.
What Rational Regulation Would Look Like
FDA’s September 2025 nicotine pouch pilot program demonstrated that rigorous and efficient review are not mutually exclusive (Tobacco Law Blog, 2025). The on! PLUS authorization in December 2025 confirmed it. Real-time applicant communication, literature-based study requirements, and focused critical element review cut timelines dramatically without any evidence of compromised standards (FDA, 2026).
That pilot should be the floor, not the ceiling. A product class with documented 95–99% lower toxicant exposure, no combustion, no inhalation, no tobacco leaf, and no serious adverse events in any trial conducted to date (Hartmann-Boyce et al., 2025) does not require the evidentiary apparatus of a novel pharmaceutical. The rest of the world has largely reached this conclusion.
In the meantime, 47.7 million Americans who smoke continue using a product that kills approximately half of them — while regulators elsewhere issue notifications, complete registrations, and authorize sales. At $201 per life saved, the U.S. PMTA process is not the problem. The problem is that it is 167 times more expensive than the alternative, without any measurable difference in the public health outcomes it is designed to protect.
_____________________________________
J. Preston Campbell, PhD, is a cancer researcher, harm reduction scientist, and co-founder of multiple companies, currently focusing on ENSO, his consulting and formulation company. His work focuses on translating reduced-risk nicotine products from laboratory science to regulatory approval and commercial deployment.
A new report highlights growing public misperceptions about nicotine products, with 59% believing that vaping is as harmful to health as smoking, a number that increases to 72% among 18–24-year-olds. The “Nicotine Product Harm Perception Report 2026,” released by Northerner and Haypp, surveyed 2,000 people in the UK, with nearly half believing vaping exposes users to more chemicals than cigarettes, and 60% registering as misinformed or uninformed when comparing nicotine pouches’ harm to smoking.
The findings point to a shift in risk perception that contrasts with established public health messaging on relative harm. The report links these beliefs to broader narratives around a perceived “vape epidemic,” with 78% of respondents agreeing such an epidemic exists despite vaping prevalence estimated at around 10% of adults. This disconnect suggests that public understanding may be shaped more by media framing and social discourse than by underlying usage data.
The report also cites inconsistent policy approaches and negative coverage as contributing factors to mixed public messaging around vaping and harm reduction. Experts warn that confusion over relative risks could affect smoking behavior. Dr. Marina Murphy, the senior director of scientific affairs at Haypp Group, said misperceptions may reduce incentives for smokers to switch to alternatives, potentially slowing or reversing declines in smoking rates.
“Alarmist messaging and negative framing risk doing real damage,” Murphy said. “If smokers are put off switching, we risk undoing years of progress in reducing smoking rates. People need clear, balanced information about nicotine products so they can make informed choices.”
How harm reduction, illicit markets, and regulatory gridlock are reshaping the future of nicotine policy in the United States
By Dave Dobbins, Principal Dobbins Consulting
It is now clear that reduced-risk nicotine delivery products such as e-vapor and nicotine pouches are accelerating declines in demand for cigarettes. One need only follow the earnings calls of major cigarette manufacturers in the United States to confirm this fact. Bonnie Herzog, an analyst with Goldman Sachs with an expertise in tobacco products, predicts ongoing declines of cigarette volume year over year through 2035 at roughly a 40% higher rate than between 2016 and 2024, resulting in a 63% decrease in cigarette sales between now and 2035.
However, Herzog predicts almost all the lost volume in cigarettes will be replaced by products with much lower risk than cigarettes such as nicotine pouches and vapor. In other words, the demand for nicotine will persist, but the risk of death and disease will be greatly reduced. On its face this seems like an obvious triumph for public health, but ironically there is an important segment of tobacco control advocacy that views this result as unacceptable.
For many years, tobacco control has focused on reducing and preventing smoking. This was a sensible goal; the cigarette is the country’s leading cause of preventable death. The emergence and popularity of reduced risk nicotine delivery options complicated the issue by separating nicotine delivery from the hazards of smoking. Both e-vapor and nicotine pouches were developed outside of the cigarette business and were very quickly adopted by consumers. Both present a small or undetectable fraction of the toxins present in cigarette smoke.
The popularity of these products presents an opportunity and a threat. Unfortunately for the development of policy around reduced risk alternatives, the first product to develop mass popularity in the United States was the e-vapor device Juul, and it became disproportionately popular with young people. Prior to the eruption of Juul in 2018 and 2019, the conversation in tobacco control around reduced-risk products had included consideration that the technology might serve as a substitute for adult cigarette smokers that would greatly reduce disease and death. Now, the major lobbying groups in United States tobacco control, the Campaign for Tobacco Free Kids, American Heart Association, American Lung Association, and American Cancer Society Cancer Action Network (“the Prohibitionists”) are all aligned in the view that all non-medicinal nicotine products should be banned. This is despite the enormous reductions in youth e-cigarette use in the years after 2019, continued low rates of youth nicotine pouch use, and youth cigarette use of 1.4% in 2024, a number that was unimaginable even ten years ago.
Youth Concerns to Broad Policies
The Prohibitionists advocate for bans of flavored nicotine products, taxation at very high levels for all nicotine products without consideration of relative risk, eliminating menthol and virtually all nicotine from combusted products, resistance to all FDA authorizations of reduced risk products, and to efforts by manufacturers to communicate true facts about relative health risks. At an international level, tobacco control leaders and the WHO, funded by Bloomberg Philanthropies, just as the Prohibitionists are in the US, call for all out bans on reduced risk products and laude countries that adopt such prohibition policies. Last year, prohibition advocates supported a UN Declaration on Noncommunicable Diseases that treated all nicotine products the same without recognizing the huge differences in risk of those products. The declaration thankfully failed to gain consensus, but the idea has not gone away.
This absolute resistance to reduced risk consumer nicotine products can no longer credibly be based on a concern that lower risk nicotine products will create a “gateway” to smoking that will result in increased youth smoking rates. In fact, the opposite has occurred and the introduction of reduced risk products has coincided with youth smoking rates dropping to previously unimaginable lows. While it is a universal goal to prevent youth nicotine usage, it is a reasonable hypothesis that reduced-risk products diverted some youth who otherwise may have taken up smoking.
Instead, calls for nicotine prohibition appear to be motivated by a belief that no entity should be able to sell nicotine for a profit because it is a dependence-inducing drug. Calls for nicotine prohibition are also motivated by a desire for retribution against cigarette companies. Lastly, the Prohibitionists argue that new reduced risk products are a ruse designed by manufacturers to hook a new generation of young people regardless of whether they progress to cigarette use.
The Prohibitionists rarely are held to account for the costs of the policies they recommend, but for policy makers to appropriately evaluate their suggestions they should be required to “show their work” regarding the impact of those policies on public health and society. While the Prohibitionists may feel their policy program is virtuous, that does not determine how the policies will play out when deployed in the real world. After all, sometimes the road to hell is paved with good intentions.
Lessons From Global Experiments
The first question nicotine prohibitionists must answer is why it will work for nicotine when it has failed to significantly reduce the supply of any other psychoactive drug. Instead, the reaction to prohibition has always been the development of illicit markets to address consumer demand. In fact, this is happening with nicotine in places where prohibition policies have been put in place. Bhutan’s attempted to ban tobacco products in 2010 but withdrew the measure in 2021 because of resulting criminality and black markets, and public outrage at attempts to enforce the law. In Australia vapor is illegal as a consumer product and the tax rate on cigarettes is so high that it is functionally a prohibition measure. The result has been a transfer of tobacco supply to criminal gangs that use violence to intimidate legitimate retailers and to protect territory from other gangs.
But we do not need to look abroad to see that prohibition does not work. In the United States, the FDA has not authorized a single flavored vapor device outside of tobacco and menthol. Yet they are ubiquitously available through unregulated black markets. Estimates are that over 70% of US vapor device purchases are illicit devices. And consumers have shown a clear preference for the features of devices in the illicit market. There have been significant seizures of illicit products and evidence of involvement of organized crime, such as Mexican cartels, but enforcement efforts have been unable to significantly impact supply just as they have been unable to significantly reduce supply of other drugs.
Second, to the extent that prohibition tactics work to reduce the supply of reduced-risk products, the inevitable result would be slowing the transition by smokers to those safer products. The grim math is that the Prohibitionists (whether consciously or subconsciously) appear willing to sacrifice lives in pursuit of eliminating “commercial” nicotine. All policies have tradeoffs, and by abandoning a focus on improving morbidity and mortality of people who smoke, excess deaths become the inevitable cost. Here the number of lives at stake is huge. When dealing with a population of 31 million people who smoke, a 5% change in switching over time is more than 1.5 million people smoking who otherwise would have switched. It may be that some advocates believe that the pursuit of a nicotine-free future is worth this sort of sacrifice, but they owe it to the public to be transparent about the tradeoffs.
Lastly, the goal of a society without “commercial” nicotine is based on a premise that people do not actually want nicotine but are tricked into using it by sophisticated marketing schemes and then become addicted or dependent and can never quit. It is certainly true that nicotine causes addiction and dependence. And advertising has undoubtedly played a part in the expansion and decline of cigarette use. However, nicotine does have hedonistic effects. For example, it improves cognitive function and moderates mood. Moreover, people have been seeking nicotine far before the advent of modern marketing. It became a major cash crop in the American South and was exported throughout the world by the 1700s. Even though they are now universally understood to cause chronic disease and illness, cigarettes are still smoked by over a billion people worldwide. Suffice it so say, there is little indication that demand for nicotine is going away in the foreseeable future.
So where does that leave a responsible government? First, while vastly reducing cigarette use is a desirable and achievable societal goal, it is highly unlikely that the elimination of all “commercial” nicotine sales is achievable. Governments that attempt to create a nicotine-free society will incur significant societal costs by prolonging smoking and shifting supply to illicit markets. If a government were to go so far as to commit to a “drug war” approach to a product like nicotine pouches, it is likely it would suffer significant reputational damage, and of course, the implementation of those enforcement strategies has its own costs that tend to fall largely on disadvantaged populations.
Once the Prohibitionists show their work, it is clear their program is impossible and destructive. The alternative is realistic regulatory measures to mitigate the risks of nicotine markets. This is how governments handle alcohol, gambling and other risky behaviors. An ideal nicotine regulatory regime would include harm reduction, but also would act to ensure product quality, limit youth use and access, and act as a trusted source of scientifically validated information. The United States currently has a structure of a nicotine regulatory regime, but the regulator has interpreted its statutory mandate to make actual regulation of the nicotine market impossible.
FDA Authority and Modern Regulation
We have heard many times from the leadership of the Center for Tobacco Products that it has simply been trying to apply the “appropriate for the public health” (APPH) standard it received from Congress in the Tobacco Control Act. However, the definition of APPH is broad, advising the agency to weigh the benefits of switching against the risks to nonsmokers. That should also include the risks of taking a regulatory approach that inevitably spawns multi-billion-dollar illicit markets that operate entirely outside the regulatory system.
CTP also must acknowledge the statutory deadlines in the Act. So far, they have been totally ignored. Reviews that should be complete within 180 days have routinely taken years. To get to a point where it can meet all its statutory obligations, CTP must switch its tobacco pre-market approval review to a much more pragmatic framework instead of the intensive multi-year review process it is currently doing on a product-by-product basis. Indeed, the statute appears to require such an approach. This should focus on real-world solutions, including:
• Establishment of baseline standards for products focusing on nicotine delivery and exposure to harmful and potentially harmful constituents
• Requiring manufacturers to register and comply with inspection
• Time, place, and manner of sale restrictions that protect youth
• Instituting a strong post-market surveillance system to ensure not only compliance but to monitor adverse events and unexpectedly high youth usage.
If a manufacturer can attest to following all these requirements, it should be allowed to market its products with the understanding that CTP has the power to revoke authorization in the event post-market surveillance uncovers problems.
This would create a regulatory system that could vastly increase manufacturer accountability to the regulator and increase the availability of regulated options for people who smoke to switch. It would also disincentivize and crowd out illicit markets. Ironically, this approach would also be more effective at dealing with youth use, the issue most emphasized by the Prohibitionists, because it allows the regulator to respond to upticks of youth use of products in cooperation with an accountable manufacturer.
The lack of regulatory authority over Juul was a major contributor to the fiasco in 2018-19. This system will not be perfect or without risk, but this is simply an area where that is an unachievable goal. Tradeoffs are inevitable. Surely, it is time to try a reality-based approach instead of pursuing an impossible goal that generates effects directly in opposition to the goals of the TCA.
At the American Tobacco and Nicotine Forum (ATNF), a panel titled “Tobacco Harm Reduction: Communicating to Adults Who Smoke” brought together public health experts, physicians, and industry representatives to examine why reduced-risk messaging is failing to reach adult smokers. Moderated by Cliff Douglas, president of Tobacco Control Law and Policy Consulting, the discussion focused on the disconnect between scientific evidence, regulatory communication, and real-world consumer understanding, with panelists pointing to a significant opportunity to better engage healthcare providers as trusted intermediaries. Douglas said the number of contrasting views from “authorities” in government and industries has eroded trust of consumers across most markets.
Dr. Mohamadi Sarkar, a fellow in regulatory affairs for Altria Client Services, emphasized the scale of misinformation, noting that many smokers believe vaping is as harmful as smoking and that nicotine pouches cause cancer—perceptions he said are not supported by current evidence. He argued that while regulators acknowledge a continuum of risk, that message is not reaching consumers due to communication restrictions and slow dissemination of scientific findings. Sarkar also highlighted that even physicians often lack awareness of tobacco regulation and product differences, suggesting that a grassroots, evidence-based approach—combined with better education of healthcare providers—could gradually shift understanding and influence patient decisions.
Dr. Mark Tyndall, an author and vaping advocate, framed harm reduction through a clinical lens, arguing that abstinence-only messaging is ineffective and that switching to lower-risk products should be treated as a pragmatic health intervention. He compared nicotine alternatives to substitution therapies in other areas of medicine, stressing that providing safer options is both ethical and necessary. Dr. Julie Gunther, a physician based in Boise, Idaho, reinforced the practical challenges physicians face, noting limited patient interaction time and a lack of nuanced education within the medical system. She said most healthcare environments do not differentiate between nicotine products, while real influence increasingly comes from peers, pharmacists, and social media. Across the panel, speakers pointed to stigma, regulatory constraints, and inconsistent public health messaging as key barriers, with calls for clearer, fact-based communication to help adult smokers make more informed choices.
At the American Tobacco and Nicotine Forum (ATNF), the panel titled “Adults Who Smoke: The Beneficiaries of Harm Reduction Reform” focused squarely on adult smokers as the primary population that stands to benefit from expanded access to reduced-risk nicotine alternatives. Moderated by Dr. Jasjit Ahluwalia, a professor at Brown University, the discussion challenged prevailing narratives in public health, particularly the strong emphasis on eliminating all nicotine use and the skepticism toward dual use. Ahluwalia argued that quitting smoking is often a process rather than a single event, and that transitional behaviors—such as using both cigarettes and alternatives—should not be automatically dismissed if they move individuals toward lower-risk products.
Panelists brought personal and advocacy-driven perspectives to the conversation. Consumer advocate Phillip Kirschberg, a consumer advocate, described how vaping enabled him to move away from a heavy smoking habit after multiple failed quit attempts, arguing that alternatives should be more readily available and not stigmatized given their potential to save lives. Consumer advocate Kim “Skip” Murray echoed the real-world nature of behavior change, noting that many smokers initially adopt alternatives situationally rather than with the explicit goal of quitting. Elizabeth Hayes, lead of external affairs for the Consumer Choice Center, emphasized that many smokers transition simply because alternatives are more appealing, adding that clearer differentiation between product categories is needed so adult consumers understand relative risks and available options.
A central theme of the panel was the gap between scientific understanding and public perception. Speakers argued that misinformation and lack of communication have left many adults believing that alternatives like e-cigarettes are as harmful as cigarettes, limiting their willingness to switch. Panelists also stressed the importance of flavors and product variety in supporting switching, while acknowledging the political sensitivity of the issue. Across the discussion, there was a consistent call for more honest, evidence-based communication, greater inclusion of consumer voices in policymaking, and a shift toward policies that recognize harm reduction as a pragmatic tool to reduce smoking-related disease—particularly for older, long-term smokers who may not otherwise quit.
British American Tobacco Chair Luc Jobin told shareholders at the company’s 2026 annual meeting that the group is making strong progress in its transformation toward a smokeless future, driven by growth in reduced-risk products and continued investment in innovation, science, and digital capabilities. He highlighted a more than 15% increase in smokeless product users in 2025 and reaffirmed confidence in BAT’s medium-term targets, including 3–5% revenue growth and 4–6% operating profit growth, despite regulatory challenges and market volatility.
“We enter 2026 with accelerating momentum, powered by a strengthened innovation pipeline, deep strategic partnerships, and growing confidence in our future-fit capabilities,” Jobin said. “This progress underpins our confidence in sustainably delivering our mid-term algorithm of [growth].”
Emphasizing harm reduction, Jobin called for evidence-based regulation to support alternatives to cigarettes and said the company remains well-positioned to deliver long-term value as it advances its strategy, despite a complex and volatile market.
“We have activated comprehensive Business Continuity Plans to mitigate potential disruption, and we are closely monitoring the situation in the Middle East as it evolves,” he said. “As of today, the conflict is not currently having a significant impact on the Group’s business.”